这是asco2014上发布的研究计划。三期了。12mg每天
A multicenter, open-label, phase 3 trial to compare the efficacy and safety of lenvatinib (E7080) versus sorafenib in first-line treatment of subjects with unresectable hepatocellular carcinoma.
Subcategory:
Hepatobiliary Cancer
Category:
Gastrointestinal (Noncolorectal) Cancer
Meeting:
2014 ASCO Annual Meeting
Session Type and Session Title:
General Poster Session, Gastrointestinal (Noncolorectal) Cancer
Abstract Number:
TPS4153
Citation:
J Clin Oncol 32:5s, 2014 (suppl; abstr TPS4153)
Author(s):
Richard S. Finn, Ann-Lii Cheng, Kenji Ikeda, Masatoshi Kudo, Toshiyuki Tamai, Corina E. Dutcus, Steven Younger, Kwang-Hyub Han, Shukui Qin, Eric Raymond; Geffen School of Medicine at UCLA, Los Angeles, CA; Department of Oncology, National Taiwan University Hospital, Taipei, Taiwan; Toranomon Hospital, Tokyo, Japan; Department of Gastroenterology and Hepatology, Kinki University School of Medicine, Osaka, Japan; Eisai, Tokyo, Japan; Eisai, Woodcliff Lake, NJ; Severance Hospital, Yonsei University, Seoul, South Korea; PLA Cancer Center of Nanjing Bayi Hospital, Nanjing, China; Hopital Saint-Antoine, Paris, France
Abstracts that were granted an exception in accordance with ASCO's Conflict of Interest Policy are designated with a caret symbol (^).
Abstract Disclosures
Abstract:
Background: Lenvatinib (L, E7080) is an oral multi-targeted tyrosine kinase inhibitor of VEGFR1-3, FGFR1-4, PDGFRβ, RET and KIT. Given the role of angiogenesis in hepatocellular carcinoma (HCC), a phase 1/2 open-label study evaluated the safety and efficacy of L in 46 patients with advanced disease and Childs-Pugh (CP) A liver function status (Kudo ILCA 2013). Patients were treated with a starting dose of L 12 mg qd (28-d cycles) until disease progression or development of unmanageable toxicities. Median time to progression (TTP) was 12.8 months (mo; 95% confidence interval [CI] 7.23–14.7) and median overall survival (OS) was 18.7 mo (95% CI 12.8–25.1). The most common adverse events were hypertension 76% (Gr3 54%), palmar-plantar erythrodysesthesia syndrome 61% (Gr3 7%), proteinuria 59% (Gr3 20%), anorexia 57% (Gr3 2%), thrombocytopenia 50% (Gr3 33%), and fatigue 48% (Gr3 0%). Overall response rate (ORR) was 37%; 45.7% had stable disease. Methods: Based on these phase 2 data, a global, randomized, open-label phase 3 trial was designed to determine if L is non-inferior or superior compared to sorafenib (S) in advanced HCC. Eligible patients (N=940) with Barcelona Clinic Liver Cancer Stage B or C HCC, CP A status, and ECOG 0-1 will be randomized 1:1 to either L 12 mg or 8 mg orally qd (based on body weight [BW]) or S 400 mg orally bid. Patients will be stratified by region; macroscopic portal vein invasion, extrahepatic spread, or both; ECOG-PS; and BW (<60 vs ≥60 kg). The primary endpoint is OS. Secondary endpoints include progression-free survival, TTP, ORR (modified RECIST criteria), safety and PK/PD. Given an estimated median OS for S of approximately 10 mo, a 2.5 mo improvement was derived to achieve a hazard ratio (HR) of 0.8. Statistical study power (using a non-inferiority test by the 95% CI lower-limit method on log HR for OS) was determined based on this HR and a non-inferiority margin of 1.08, corresponding to 60% retention of S effect vs placebo. Based on these assumptions, the study power to declare non-inferiority or superiority is approximately 97% and 82%, respectively. The overall false positive rate is 0.05 (2-sided). Clinical trial information: NCT01761266. |
 爸爸晚期肺癌肿瘤已经看不到了!我确
讲述者:陈先生整理者:pear
适逢暑假得闲,我带着全家自驾出游,正将最后一件行李塞
爸爸晚期肺癌肿瘤已经看不到了!我确
讲述者:陈先生整理者:pear
适逢暑假得闲,我带着全家自驾出游,正将最后一件行李塞
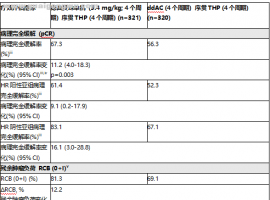 DESTINY-Breast11 III期临床研究
DESTINY-Breast11 III期临床研究:优赫得序贯THP方案术前治疗,使高风险HER2阳性早期
DESTINY-Breast11 III期临床研究
DESTINY-Breast11 III期临床研究:优赫得序贯THP方案术前治疗,使高风险HER2阳性早期
 MATTERHORN III期试验中,与单独化疗
MATTERHORN III期试验中,与单独化疗相比,英飞凡治疗方案将早期胃癌患者死亡风险降低
MATTERHORN III期试验中,与单独化疗
MATTERHORN III期试验中,与单独化疗相比,英飞凡治疗方案将早期胃癌患者死亡风险降低
 跨越十年丨憨叔靶向轮换的感悟及思路
我们在筷子治疗九周年纪念文章《跨越九年丨憨叔靶向轮换传承和发扬 --筷子奥希替尼
跨越十年丨憨叔靶向轮换的感悟及思路
我们在筷子治疗九周年纪念文章《跨越九年丨憨叔靶向轮换传承和发扬 --筷子奥希替尼
 母亲晚期肺癌跨越13年,这是我家长期
讲述者:不怕辣椒不怕癌整理者:雪漓
在我家抗癌跨越10年之际,鹰版就曾邀请我写一篇
母亲晚期肺癌跨越13年,这是我家长期
讲述者:不怕辣椒不怕癌整理者:雪漓
在我家抗癌跨越10年之际,鹰版就曾邀请我写一篇



 显身卡
显身卡


